

When the "misinformation gurus" promote misinformation...finding fault with "Faultlines"
A response to the document published in January by the Council of Canadian Academies


This is my personal response to a study published in late January entitled: “Faultlines. The Expert Panel on the Socioeconomic Impacts of Science and Health Misinformation”
The document was published by the Council of Canadian Academies (CCA - 2 C’s).
The report includes a model of the impacts of COVID‑19 misinformation on vaccination rates in Canada, producing quantitative estimates of its impacts on our health and the economy, and situating these within a broader context of societal and economic harms.
The members of the Scientific and Medical Advisory Committee of the Canadian Covid Care Alliance (CCCA - 3 C’s) have published their formal response here: https://www.canadiancovidcarealliance.org/wp-content/uploads/2023/02/23FE6_CCCA-response-to-CCA-misinformation-report.pdf
My response comes from my perspective as a retired educator and a decades long health advocate for a handful of friends and family members. The thoughts I share here are my own, based on my having “followed the science” since early 2021. Already in March of 2021 key findings were becoming known in the scientific literature — thanks to the Japanese government pressing Pfizer to release information about where in the body the vaccine components were tracked to migrate, aka “bio distribution.” This article on what it means to follow the cyclical nature of the Scientific Method, shares some of these key findings from early 2021.
Months later, Alberta’s former provincial Chief Medical Officer of Health of Alberta, Dr. Deena Hinshaw, filed documentation before the courts. I was appalled to note how little of this information from the field she was aware of!!! I then tried to track how she was being informed to support her decision making when it came to COVID mitigation measures. I posted my findings online: FOLLOWING THE SCIENCE - Documenting the Current State of Affairs of COVID-19 Vaccination in Canada as of October 21, 2021. (Click here for the table of contents to the entire compilation and hear specifically for my “think aloud protocols” as I “followed the science” within various documents/sources.) That was followed up with many letters to decision makers, including science advisors, politicians, school board chairs etc. which can be accessed further down on this page: https://followingthecovidscience.8b.io. Over TWENTY MONTHS ago, I addressed a letter to the chairs of Alberta’s Scientific Advisory Group (SAG) as it was rapidly becoming clear that the CMOH was relying directly on their guidance, yet the documents provided by the SAG were not on the cusp of a very rapidly moving field. This link will let today’s readers know how much information was ALREADY KNOWN in the field but apparently/possibly? KEPT FROM our decision makers already in mid 2021 - BEFORE many of the government mandated vax-rollouts.
~~~~~~
One would think, in order to be taken seriously, any analysis on COVID vaccine hesitancy and the costs to the health care system of NOT having everyone step in line to roll up their sleeve as per government directives, would include among its authorship people who are experts in the fields of microbiology, virology, vaccination, and front line hospital care. Instead, the 13 experts listed as the authors of this much vaunted study on vaccine “misinformation” come from a number of corners of the new field of “COVID misinformation studies” and would have a lot to lose if their entire field were to be suddenly debunked!
The authors of the recent report by the CCA include a health care economist; a second economist with a background in agricultural supply chains (and consumer perceptions around novel food and agricultural technologies as well as “challenges and best practices in communication about novel technologies, in particular agricultural biotechnology”); a cognitive psychologist; a professor of information and communication; a former Research Manager on Facebook’s Central Integrity team with experience “protect[ing] people and communities from harmful experiences on Facebook”; a journalist who pursued university studies in sociology and history but who has a “strong interest” in science writing; 2 people with Bachelor of Science degrees (one who followed that up with 2 law degrees and who now focusses on “the public representations of science and public health policy” and the other who followed their BSc (in Business Management) with an MA in International Relations and a Juris Doctor in International Law. This latter person has two decades of experience working in communications, marketing, and business management in domains such as academia, high-tech and politics.
Also on the committee was an expert with a background in the “architecture of ideas" Canada Research Chair in Digital Communication for the Public Interest. Her government funded research examines “the ways that misinformation can be mitigated through digital communication efforts, particularly those targeted at the research community”. It is the lingo coming out of this person’s field with wording such as “educational interventions to address COVID-19 related misinformation, … the discourses of conspiracy theories, and ecological approaches to understanding misinformation in a modern context” that is reflected throughout the document the committee recently produced.
Of the 13 committee members, only one appears to be a practicing primary care physician with eyes on the ground when it comes to direct patient experiences, symptoms and treatment. And one is a professor of paediatrics - however, she appears less focused on the biomedical processes engaged when vaccines are injected into a child’s body and chooses instead to focus on “vaccine safety, hesitancy, pain mitigation, education and policy including consulting work with the World Health Organization.” Yet another health professor on the committee has a focus on anti-stigma interventions in mental health delivery, and the use of community health centres in the delivery of addictions and mental health services as well as in the international human right of access to health care.
This committee was chaired by a former professor of sociology, decades long civil servant and highly engaged citizen with involvement in initiatives to end homelessness and to support wildlife.
My first set of questions for the board of the Canadian Council of Academies is:
Given your statement: The members of the expert panel responsible for the report were selected by the CCA for their special competencies and with regard for appropriate balance. HOW DID YOU DETERMINE THE SCOPE OF REQUIRED “COMPETENCIES” and WHY DID YOU EXCLUDE INDIVIDUALS WITH EXPERTISE IN COVID-19 MITIGATION, PREVENTION, TREATMENT, ETC. FOR A DOCUMENT ON INFORMATION/MISINFORMATION ON COVID? Would you hire gardeners when it comes to heavy equipment repair work? HOW DID YOU EXPECT COMMUNICATION SPECIALISTS WITH LITTLE SCIENCE BACKGROUND TO QUICKLY ATTAIN THE SCIENTIFIC COMPETENCE TO BE ABLE TO ASCERTAIN THE VALIDITY OF EXPERT SCIENTIFIC FINDINGS? i.e. how were the gardeners supposed to quickly learn everything needed to be able to supervise the heavy duty equipment mechanics?
Please note: my critique of the committee members shared here is by no means intended to diminish their standing as competent and likely compassionate and dedicated individuals. I am sure if I could meet them, we would have lots in common and plenty to talk about as fellow concerned Canadians. But rather, by pointing out their focus on “misinformation studies” and “data modelling” to the complete EXCLUSION of all information on “COVID studies” I am writing to ask you to commission a second panel, chaired and composed of top Canadian academics in the fields actually related to the topic at hand.
I am noting that over the entire 150+ pages of the report, there is no section in which the authors looked at any of the “data in context” that currently makes up the information/evidence/knowledge in the field of COVID care and mitigation. I wonder then, how their conclusions are supposed to be relevant and meaningful to the task at hand. (To continue with my metaphor, findings about the pistils inside a blooming tulip don’t help me repair the pistons of the hydraulic pump of our company backhoe.) Just as there is little that PISTELS have in common with PISTONS, except on a superficial level - a few letters of the alphabet - there really is NOTHING in common with the way the phrase “ COVID-19 INFORMATION” is understood by experts in the field of “misinformation studies” and the way that same phrase is understood by experts in the field of “COVID studies". It is 100% evident that if the Council of Canadian Academies wished to retain its reputation as a solid & reputable organization, it will need to convene a second panel and produce a second report. If you fail to do so, global evidence gathered on COVID-19 vaccine products, will rapidly demolish the recent Faultlines publication and with it, the prestige of the CCA.
The self-congratulatory tone of the document - showing how corporate social media fact checkers were able to play “gotcha” with leading world experts, and the absolute unawareness of the authors of the mountains of evidence gathered globally, both evoke revulsion and disgust in the minds of educated readers.
Devoting endless pages of the report on people’s attitude toward vaccination based on pre-2019 innoculations, or even the socioeconomic differences in C-19 vaccine uptake early in 2020 does not solve our current situation now — that repeat COVID-19 infections, the meteoric rise in excess mortality, sudden deaths, adverse events, etc, etc. are now known to be dose dependent. Now, when peer-reviewed specialists are determining that there are ways in which spike protein bonds to the ACE-2 receptors in key cell types in the body can be reversed and now that physicians are currently STILL blocked from having access to treatment protocols WHILE INJECTIONS STILL CONTINUE AND THE EXCESS DEATH RATES STILL CLIMB (except in uninfected segments of the population.) Now, when even Canada’s National Advisory Committee on Immunization (NACI) has removed everyone under age 65 from their recommended vaccine targets but this is not being communicated to the public…
Sadly, the report’s conclusions are being used by those with a stake in keeping the false “safe and effective” narrative going, to attack those who truly “follow the science” around the SARS CoV-2 virus, the types of immunity, the adverse effects induced by mRNA injections and the care of COVID patients.
My second set of questions for the board of the Canadian Council of Academies is:
WHAT WERE THE TERMS OF REFERENCE GIVEN TO THE PANEL MEMBERS FOR THE SCOPE OF THEIR REPORT? WHICH TIME FRAME & WHICH IMMEDIATE PROBLEMS WERE THEY DIRECTED TO FOCUS ON? WERE YOU AS THEIR “CONTRACT HOLDERS” AWARE OF THE HUGE SHIFT THAT OCCURRED IN EARLY 2021 WHEN IT CAME TO THE JAPANESE PFIZER BIODISTRIBUTION STUDY?
If you as the Board members who initiated this publication are not yourselves aware of the basic architecture of the knowledge within the field of COVID vaccine studies, then you will not be able to recognize whether or not the writers you engaged were able to provide you with quality work or with crap. Sorry for the crass word use, but both gardners and mechanics would “tell it like it is” when they see the opposite of quality work!
So please allow me to introduce you to just a few key aspects of the field of COVID-19 vaccine studies, since it appears these were missed in the directions which those who initiated the study passed on to those who were to carry it out.
I will focus on just a) and b) knowing that as reputable academics, CCA members should be able to follow the remaining points on their own! (Er…. they should have been able to do so for the last 2 years without my letter, but hey, we all gotta start somewhere in the attempt to slip out from under the grip of censorship!)
To understand COVID-19 studies, one needs to be aware of….
a) clear definitions of terms. (I will limit myself to the public health definitions of information, etc. This topic should be expanded to include redefinitions of key concepts like “pandemic”, “vaccine”, “herd immunity” etc. - redefinition that are suspect in their timing for starters.)
b) the monumental paradigm shift that occurred with the release of the Pfizer bio distribution data to Japan in early 2021, as noted above
c) the court ordered release of Pfizer data in March 2022
d) the release of the Twitter files made possible by Elon Musk, showing the illegal collusion between the US regulatory agencies and at least one of the social media platforms - to effectively SILENCE global EXPERTISE in order to falsely claim that NO OTHER ALTERNATIVE TREATMENTS for C-19 exist, thus allowing BigPharma’s profit machine to benefit from (fraudulently) being granted emergency use authorizations, etc. (For a brief taste of this topic, please view this short clip in which Twitter executives are grilled by US Congresswoman Nancy Mace.)
e) the recent release in the UK of the correspondence to and from former British Health Secretary Matt Hancock, showing how he nonchalantly discussed “deploying” new variants when uptake of injections wasn’t following according to plan and the people needed a new dose of fear factors.
f) the near weekly revelations from top level officials at Pfizer/Moderna/the FDA/the CDC including those up in the yellow “sticky” in the graphic above, so many HUGE revelations to come out in just 2-3 days - nothing of them in mainstream media and nary a peep coming from our “misinformation gurus” who, we believed are working for publicly funded institutions of knowledge and should at the very least make knowledge clear to the public!
All of the information mentioned follows a steady stream of near daily publications of peer-reviewed scientific studies which the international scientific community followed closely, pooling expert knowledge to jointly build understanding of this field, unbeknownst to followers of “Covid misinformation studies.”
Clearly the panel members missed these major revelations in the field of COVID studies. Much before September 2022, it was obvious that those who professed the “safety and efficacy” of the C-19 vaccine products were themselves pimping misinformation. But it took me till September to post examples of evidence of which your panel members were likely totally unaware - evidence that calls us to “flip the switch” on what we consider “Misinformation”. I invite you to skim this over to expand your background knowledge in the field.
Tufts university professor Dr. Olaf Dammann, writing from a public health - not a “misinformation studies” perspective - provides a clear look at the terms ”data”, “information”, “evidence”, “knowledge” and “beliefs” which I link to here in order to provide us with useful guidance.
Given that the term “misinformation” was not specifically defined in the Faultlines document, I went elsewhere: Misinformation can be defined “as as any testable claim that is contrary to current evidence, noting that evidence can change and that where evidence is emerging, discordant or where a claim cannot be tested, misinformation often relies on experts and expertise” (Vraga and Bode, 2020b). (Source)
Given then, that the “safe and effective” narrative supported by the CCA panel is contrary to current evidence, those who continue to share their belief in the safety, necessity and efficacy of Covid-19 injections themselves turn into purveyors of misinformation.
OUCH! Let’s look for a different definition of “misinformation” to see if that helps. 2020 was obviously a pivotal year in “misinformation studies” as the Harvard Kennedy School (hmmmm) launched the inaugural edition of a new journal: MisInformation Review. A wide-ranging definition of “misinformation” that everyone involved could agree upon was developed: (The numbers in bold are my additions, you will see why below.)
For the scope of this publication, we use the term “misinformation” to refer to all kinds of false or inaccurate information, independently from the fact that such information was deliberately created and spread to deceive. (1) Then, misinformation can take many forms. It can be a coordinated, online campaign that targets fragile communities with false or misleading information for political or economic gains. (2) A “misinformed public” can hold a series of misconceptions about a natural phenomenon, because of fear, lack of knowledge, or identity dynamics. (3) Artificial intelligence (AI) can play a big role in the diffusion of misinformation, or it can be irrelevant. A misinformation campaign can start offline and get amplified online, or vice-versa. Often, both mainstream and fringe media can help this amplification process (voluntarily or involuntarily). Pieces of misinformation can spread fast or gain traction over time. They can quickly lose relevance and have limited impact on behavior, or endure for long periods of time. Misinformation can be promoted widely, (4) or be hidden in closed, invite-only groups. One thing is certain: misinformation is a messy, old problem, that got even messier with the widespread adoption of the Internet and information technologies.
It seems unreasonable to think that we will ever eradicate misinformation for good, online or offline. Indeed, we might agree that lies and deceptions are integral parts of human communication. What we can do, instead, is to work together to build and maintain a response strategy (or multiple, parallel ones) that can to some extent prevent or reduce harmful lies and deceptions from spreading unchecked, keeping misinformation to an “acceptable level” (whatever that might look like). Of course, such a strategy requires interventions at many levels: legal, political, financial, infrastructural, cultural, and social. (5) The goal of the HKS Misinformation Review is to peer-review, share, and organize empirical, specialized research on all aspects of misinformation, which will help us conceptualize and design what this strategy might be. (Source)
(1) Note the court ordered release of Pfizer trial and implementation data back in March 2022 - 50,000 to 80,000 pages a month. What it shows is deliberate actions taken by Pfizer to hide high death rates in order to deceive the population. This further evidence that the “safe and effective” narrative is misinformation. (Source 1) (Source 2)
(2) One of the saddest things I saw in the summer of 2021 was this document distributed (I assume) to First Nation communities.

I had been reviewing the studies that were included and excluded by the BC Ministry of Health on COVID-19 treatment and prevention protocols and was well aware of Dr. Meryl Nass’ listing of the myriad ways in which at least one key safe and effective therapeutic was being suppressed in order to make way for the emergency use authorization of the mRNA and other C-19 vaccine products. With much coverage on the need for action re: past harms to Indigenous peoples that summer, I was saddened by this full-on misinformation campaign targeted at these vulnerable communities. Canada could have been a leader had we allowed preventative therapeutics to be tried out and documented in our remote communities as they had been in various other countries outside of the mainstream media bubble’s notice. When will we need our next Day of Remembrance and when will the next prime minister be pushed to apologize for harms done, against Indigeouns and non-Indigenous communities alike, for pushing the toxic vax and for NOT doing their own diligent research into these products?
(3) We continue seeing this as we note people continuing to mask while alone in their cars or while riding bikes for example. And sadly, we note some folk continuing to get booster shots - all unaware of the ‘debunked’ nature of the studies our public health officials were originally claiming to reference as they drilled these behaviours into us. Clear examples of fear and lack of knowledge.
(4) Yup, 24/7 via radio, TV, internet, billboards, public pronoucements, etc. TV producers were even given scenario ideas so that they could script pro-mask and vax messaging into sit-coms, etc.
(5) Sadly, another shortfall of the Faultlines document is the lack of strategies for teaching the population the new evolving research-based health measures that come to us via researchers and clinicians involved directly with patient care or biomedical research. (No one is informing citizens about the ways to reduce spike protein toxicity, to boost the injured immune system, to test for subclinical myocarditis, to have live blood microscopies done, etc. One would think that this committee would have been tasked to make actionable recommendations to move our country forward in this matter.)
My third set of questions for the board of the Canadian Council of Academies is:
GIVEN THAT A THIRD PARTY (THE POLLING FIRM ABACUS DATA) WAS ENGAGED TO PROCESS DATA, WHAT MEASURES WERE TAKEN TO ENSURE THAT THE STAFF WAS QUALIFIED TO UNDERSTAND HOW TO READ AND INTERPRET ADVERSE EVENTS DATA? WHY ARE THERE ZERO REFERENCES IN THE REPORT TO THE MOST COMPELLING ISSUE OF OUR TIME? - C-19 vaccine induced adverse events? WHAT THE FLIP IS GOING ON WITH THE SET-UP of the MODELLING EXCERCISE THAT MAKES UP THE BULK OF THE REPORT?
So David Collotto, the political scientist, pollster and CEO of Abacus Data was engaged to model three scenarios - completely without reference to the largest adverse event databases on the planet (VAERS, EUDRAVIGILENCE, the YELLOW CARD - none of which show up in the document????!!!!) Has Dr. Collotto heard of the Bradford Hill Criteria against which to determine a plausible causal link between the reported injury and the injection? Does anyone on the panel know about this? What about the difference between relative and absolute risk reduction? Collotto and the rest of the committee could learn a lot about pulling meaning from provincial, territorial and federal data sources by learning from data analysis’s like Sheldon Yakichuk, David Dickson (cyber crimes investigator), and Dr. William Makis to start with.
We all shake our heads when we try to follow the logic of the simulation that was cooked up by Collotto or some of the Panel members. It reads much like the science fiction that oozes its way out of pandemic simulations such as Event 201, and others - often with more economic and sociological experts and corporate leaders present than representatives of actual front line health care workers.
We read from the CCA report:
The model simulated the behaviour of people in Canada aged 12 and over between March 1 and November 30, 2021, tracking them through two waves of the COVID-19 pandemic. The model centred on whether people in Canada believed COVID-19 was a hoax and/or that vaccine harms have been covered up, drawing on the best available survey data. (6) Consistent with the published evidence, it was assumed that these two streams of COVID-19 misinformation would contribute to vaccine hesitancy. (7) The Panel then examined three hypothetical scenarios. The first scenario looked at what happens to COVID-19 vaccination rates and case numbers if the proportion of people who agreed with the statement “COVID-19 is a hoax and/or exaggerated” were vaccinated as soon as they became eligible. (8)
The second scenario looked at rates and case numbers if the proportion of people who agreed with the statement “vaccines cause many problems that are covered up” were vaccinated as soon as they became eligible. (9)
The third scenario modelled what would have occurred if everyone in Canada were vaccinated as soon as they became eligible. (10) The baseline model used real-world Canadian data. To calculate the impact of misinformation, baseline model results were subtracted from the results of each hypothetical scenario in terms of the number of vaccinations, cases, hospitalizations, intensive care unit (ICU) visits, deaths, and hospitalization costs.
If those who reported believing COVID-19 is a hoax were vaccinated when they became eligible, over 2.3 million additional people in Canada would have been vaccinated, resulting in roughly 198,000 fewer cases, 13,000 fewer hospitalizations, and 2,800 fewer deaths from COVID-19 between March 1 and November 30, 2021. (11) The cost of hospitalizations, including ICU visits associated with these cases, was conservatively estimated at $300 million. Estimates of the reductions in caseloads, hospitalizations, and deaths for all scenarios are reported in Chapter 4.
(6 & 7) Why not account for the growing number of well informed Canadians who “followed the evidence” and committed not to take any (or any more) shots based on the principle of fully informed consent? For a study published in 2023, the lack of this possibility - that evermore Canadians are refusing high risk for very little benefit - points to a remarkably uninformed study design team/panel membership.
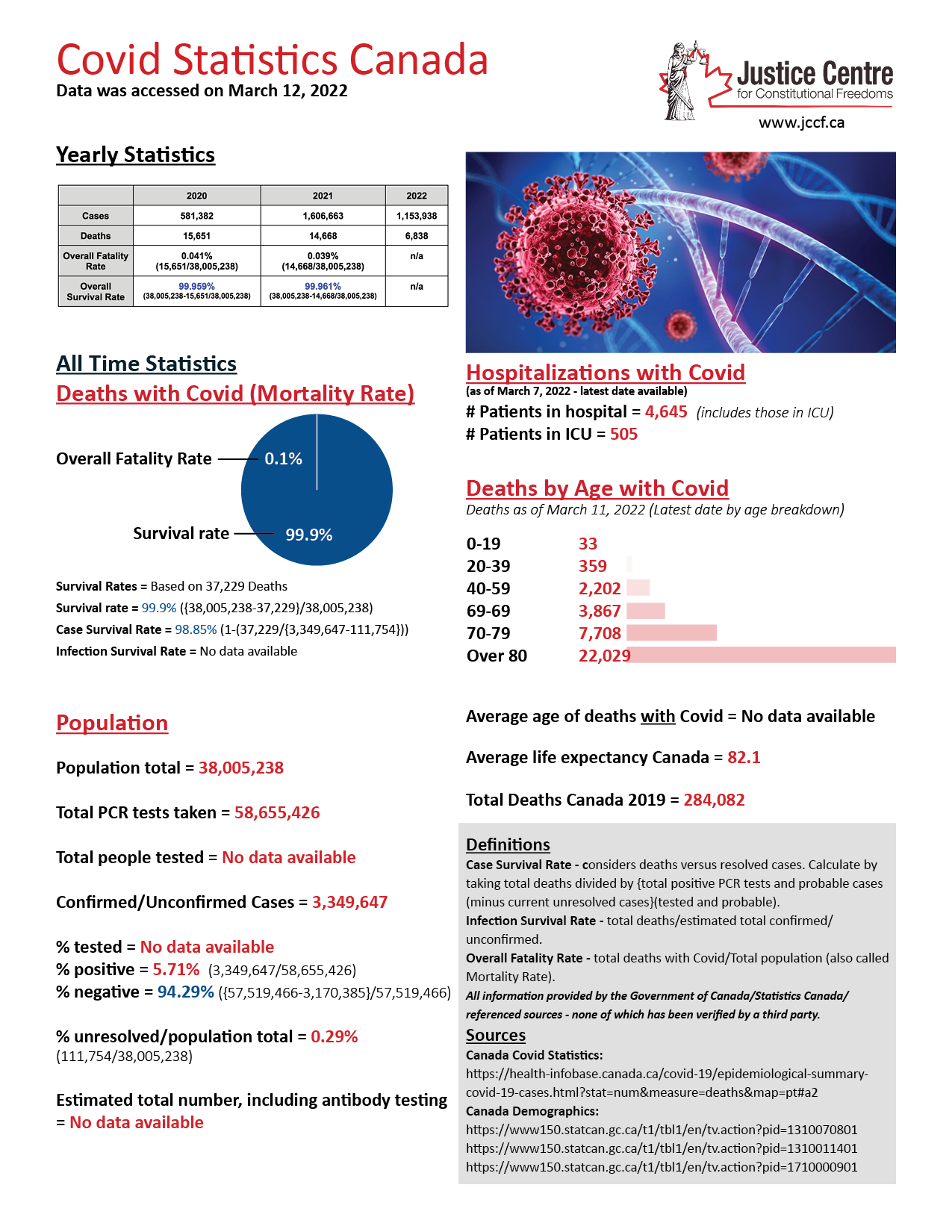
(8) So by which means of wishful thinking was the committee hoping to inform this group of Canadians that the pandemic was NOT A HOAX? The use of the word hoax implies a total lack of willingness on the panel’s part to really listen to why Canadians questioned the legitimacy of this pandemic - not the least of it was the very low COVID fatality rate among anyone younger than 75. Even a year AFTER your simulated date, Canadians were finding that the overall fatality of COVID-19 infections was 0.1% with the survival rate at 99.9%. (Source)
{kind=link}
(9) Ditto. By which means of wishful thinking was the committee hoping to counteract the growing awareness of the very real risk of vaccine harm? How could committee members expect to get compensated for what would simply amount to fiction: ‘… and then one day…puff! all the people realized that the illnesses their friends and family members were reporting post-vax were just a dream, so they went on to get their shots too…. The end!’
Taxpayer monies would be better served at having committee members such as those on this panel turn their focus the other direction! How can those who promoted the vax now face the strong regret at it having harmed fellow family members, friends or employees? What if 7 of your close family acquantences were to die within a three month period, family members who TRUSTED your take on these products and whose lives are now extinguished? And on top of that what if a close family member were to face debilitating side effects, and/or possibly go blind, 5 or 6 months later?
(10) So the committee toyed around with a 100% compliance model? in Late 2022? Early 2023? This thought speaks volumes about the committee’s total lack of awareness about fully-informed and voluntary consent provisions in public health policy. And even about the possibility of allergic reactions, not to mention the complications that serverly ill pepeople need to try to avoid in terms of vaccine harm on their fragile systems.
(11) Here we shake our heads once again at the committee’s total lack of awareness re: the 14 day period within which injected individuals are counted as unvaccineted when in fact they are at the highest risk of adverse events without anyone thinking to give them preventative treatments. We also note a complete LACK OF AWARENESS of the dose-dependent nature of the COVID-19 injections, i.e. the more often the person is injected, the higher the risk of hospitalization and death. Hospital overcrowding is traceable to the numbers of triple or quadruple injected patients as well as the sharp increase in sick leaves for frontline health workers.
The document produced does not look at all like a dispassionate analysis of policy alternatives when it comes to Covid-19 injections, which is what one should have expected - no comparison of the costs to the economy of Covid-19 vaccination versus low-cost, safety-vetted early treatment protocols. There is no mention in the report of the rapidly evolving scientific evidence that is being followed across Canada and internationally by academic physicians and other published scientific researchers on matters such as
how endothelial dysfunction contributes to COVID-19-associated vascular inflammation and coagulopathy
on the role that Autophagy can play in Spike Protein Induced Neurotoxicity
just to name a few.
Given that the Council of Canadian Academies convenes the “best experts in their respective fields to assess the evidence on complex scientific topics of public interest to inform decision-making in Canada” there should be ZERO TOLERANCE for CCA members expressly rejecting the work of their fellow Canadian academics in other fields more related to the topics at hand. The Canadian Council of Academies document includes reference to an AI program flagging a Canadian Covid Care Alliance tweet as misinformation. What a total disregard for the investigative skills of your fellow academics across the country working in fields and on problems that the panel members do not (yet) understand.
Instead of claiming outright that to count up “sudden and unexplained” deaths in the young is to engage in conspiracy theories, and instead of shaming, silencing or gaslighting those who report vaccine injuries, the “information experts” of the CCA should be seeking ways to disseminate the ever evolving knowledge around all things COVID related. One example would be teaching physicians, patients, politicians and the general public to be aware of these vaccine related neurological complications:
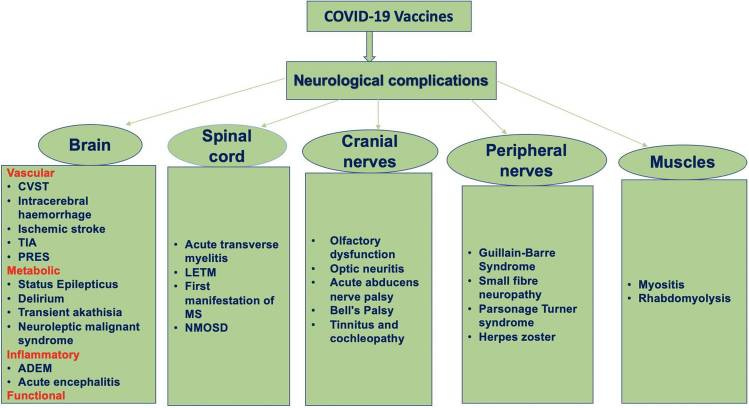
Spectrum of neurological complications following COVID-19 vaccination A flow diagram depicts the spectrum of severe neurological complications following COVID-19 vaccinations (ADEM, acute disseminated encephalomyelitis; CVST, cerebral venous sinus thrombosis; LETM, longitudinally extensive transverse myelitis; MS, multiple sclerosis; NMOSD, neuromyelitis optica spectrum disorders; PRES, posterior reversible encephalopathy syndrome; TIA, transient ischemic attacks). (Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8557950/
Having mainstream media and “official” government funded scientists such as the authors of Faultlines callously shove the increasing Adverse Event reporting under the carpet, thoughtlessly accusing eager acceptors of the vaccination drives of being “Anti-vaxxers” has been absurdly Kafkaesque. This is completely counter to the stated mission of the Council of Canadian Academies:
The Council of Canadian Academies (CCA) convenes the best experts in their respective fields to assess the evidence on complex scientific topics of public interest to inform decision-making in Canada.
The Faultlines document certainly does not reflect the work of “the best experts in their respective fields” nor does it “assess the evidence on complex scientific topics of public interest” in any way that can “inform decision making in Canada.”
Our government funded Council of Canadian Academies, instead of ensuring that the world-class COVID-19 research findings are made widely known across the nation, have produced what amounts to a mind-control, or propoganda document. The focus is on techniques used to “increase positive behaviours” and in the mind of the panel, such behaviours refer to making the choice to get injected instead of the regular supplementation with Vitamin D and other supplements to change the ph balance in the body, making it less comfortable for spike protein to maintain a hold.
I leave you with this clip in which Twitter censors are asked about their medical and scientific expertise - by which means were they of the belief that they had the subject-specific wherewithal to withhold life-saving information provided by top-tier medical experts from the population?

Likewise, what gives the CCA board members as well as the authors of the Faultline document the credibility AND expertise needed to be able to ascertain that leading and highly trained Canadian experts in the fields related to the study of SARS-CoV-2, the biochemical processes that make up the immune system, issues around spike induced neurotoxicity and ways to mitigate that, etc. etc. is to be KEPT FROM the Canadian public? Please compare the bios of your panel with that of the signatories of any one of the many documents published by the members of the Scientific and Medical Advisory Committee of the Canadian Covid Care Alliance, as seen on pages 6 & 7 here: https://www.canadiancovidcarealliance.org/wp-content/uploads/2023/02/23FE6_CCCA-response-to-CCA-misinformation-report.pdf
While the CCA panel members were theorizing how “misinformation” such as the advance planning of the pandemic and how ivermectin cures COVID is detached from or denies reality (rating these points along a continuum along with theories that Elvis & Michael Jackson are still alive, that alien abductions are real, etc.) the actual COVID information experts know where to look and how to read real data. They see the excess mortality data in every age group in temporal correlation with the mRNA vaccine product roll out. They have long been aware of what the insurance agents and embalmers have been reporting. They perform autopsies and interpret blood microscopy data. They can see the current and impending collapse and demolition of our health care system, due to the Pandemic of Vax-induced Spike Protein damage, wiping out significant numbers of the medical profession. That alongside of every other industry that continues with ongoing mandates for its workers to be “up to date” where the prevention & treatment information continues being withheld from the mainstream media bubble. Instead of needing tulip planting gardeners to pretty up the place, we are in dire need of heavy duty mechanics to do some heavy duty repairs for the health and wellbeing of us all.
It is high time that the board of the Council of Canadian Academies convenes a new panel - not on MISinformation but on actual information re: COVID-19, LongCOVID, COVID-vax induced adverse events and deaths and their prevention. Start here: https://www.canadiancovidcarealliance.org/contact-us-step3/
Thank you!
Concerned Citizen